A 35-year-old man undergoing evaluation for palpitations asks about how heart muscle cells generate an electrical impulse. Which ionic movement is primarily responsible for the steep upstroke (phase 0) of the ventricular myocardial action potential?
A. Gradual outward movement of sodium
B. Inward movement of potassium
C. Sudden inward movement of sodium
D. Slow outward movement of calcium
E. Rapid inward movement of calcium
Answer
C. Sudden inward movement of sodium
Detailed discussion for MRCP
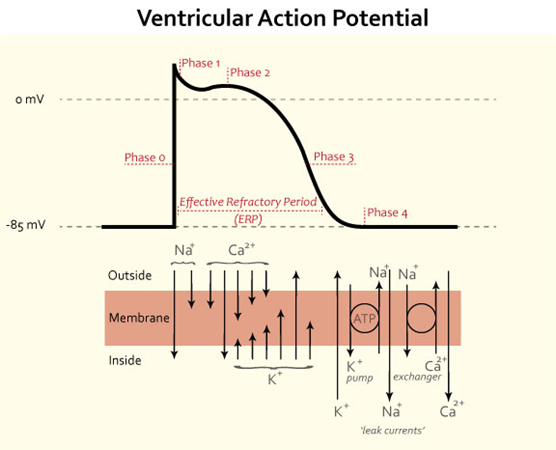
The ventricular myocardial action potential is a carefully orchestrated sequence of ionic movements across the cardiac myocyte membrane. The rapid depolarisation phase (phase 0) is driven by the opening of fast voltage-gated sodium channels, allowing a sudden influx of sodium ions (Na⁺) into the cell. This causes the membrane potential to shift rapidly from approximately −90 mV toward positive values, producing the steep upstroke seen on the action potential graph.
These fast sodium channels open when the membrane potential reaches a threshold (around −70 mV) and inactivate within milliseconds. This rapid activation–inactivation cycle explains both the speed of depolarisation and the absolute refractory period that follows. Clinically, this is crucial: any factor that reduces sodium channel availability (e.g. hyperkalaemia, class I antiarrhythmic drugs, ischaemia) will slow phase 0, reduce conduction velocity, and predispose to re-entry arrhythmias.
It is important to distinguish ventricular myocytes from pacemaker cells (SA and AV node). In nodal tissue, phase 0 is mediated by calcium influx, not sodium. This distinction is a favourite MRCP trap.
Potassium efflux is dominant in repolarisation phases (phases 1 and 3), while calcium influx during phase 2 creates the plateau phase, prolonging contraction and preventing tetany—one of the defining physiological differences between cardiac and skeletal muscle.
Conduction velocity across cardiac tissue correlates strongly with the slope of phase 0. This explains why Purkinje fibres (with abundant fast sodium channels and large diameter) conduct impulses extremely rapidly, ensuring synchronous ventricular contraction.

Cheat sheet
- Phase 0 (ventricular myocyte): rapid sodium influx
- Ion channel: fast voltage-gated Na⁺ channels
- Function: initiates depolarisation and impulse propagation
- Conduction velocity ∝ slope of phase 0
- Reduced Na⁺ channel function → slowed conduction
- Phase 1: transient potassium efflux
- Phase 2 (plateau): calcium influx via L-type channels
- Phase 3: potassium efflux → repolarisation
- Phase 4: resting membrane potential (−90 mV)
- SA/AV node phase 0 = calcium, not sodium
- Class I antiarrhythmics act on sodium channels
- Hyperkalaemia reduces Na⁺ channel availability
- Cardiac muscle contraction lasts 10–15× longer than skeletal muscle
Flash cards
Q1: Which ion causes phase 0 depolarisation in ventricular myocytes?
A: Sodium
Explanation: Fast voltage-gated Na⁺ channels open abruptly.
Q2: Which phase determines conduction velocity?
A: Phase 0
Explanation: Steeper upstroke = faster impulse propagation.
Q3: Which ion mediates phase 0 in SA node cells?
A: Calcium
Explanation: Pacemaker cells lack fast sodium channels.
Q4: What is the resting membrane potential of ventricular myocytes?
A: About −90 mV
Explanation: Maintained mainly by potassium permeability.
Q5: Which phase produces the plateau?
A: Phase 2
Explanation: Balance between Ca²⁺ influx and K⁺ efflux.
Q6: Why is tetany prevented in cardiac muscle?
A: Prolonged plateau phase
Explanation: Long refractory period prevents summation.
Q7: Which channel is targeted by class I antiarrhythmics?
A: Sodium channel
Explanation: They reduce phase 0 slope.
Q8: What happens to phase 0 in hyperkalaemia?
A: It becomes slower
Explanation: Sodium channel inactivation increases.
Q9: Which tissue conducts fastest?
A: Purkinje fibres
Explanation: Large diameter, abundant Na⁺ channels.
Q10: Which ion dominates repolarisation?
A: Potassium
Explanation: Outward K⁺ current restores negativity.
Q11: Which phase corresponds to early repolarisation?
A: Phase 1
Explanation: Transient outward K⁺ current.
Q12: What triggers opening of sodium channels?
A: Threshold membrane potential
Explanation: Usually around −70 mV.
Q13: Which phase is prolonged in ischaemia?
A: Phase 3
Explanation: Altered potassium handling.
Q14: What maintains phase 4?
A: Potassium permeability and Na⁺/K⁺ ATPase
Explanation: Resting ionic gradients.
Q15: Which drug class slows AV nodal conduction?
A: Calcium channel blockers
Explanation: AV node relies on Ca²⁺ currents.
Q16: Why does sodium efflux not cause depolarisation?
A: Efflux removes positive charge
Explanation: Depolarisation requires inward current.
Q17: Which ion movement initiates contraction?
A: Calcium influx
Explanation: Excitation–contraction coupling.
Q18: Which phase corresponds to absolute refractory period?
A: Phases 0–2
Explanation: Sodium channels are inactivated.
Q19: Which electrolyte abnormality mimics sodium channel block?
A: Hyperkalaemia
Explanation: Inactivates Na⁺ channels.
Q20: Which phase is absent in skeletal muscle action potentials?
A: Plateau phase
Explanation: No sustained Ca²⁺ influx.
MCQs to test yourself
- The ionic basis of phase 0 in ventricular myocardium is:
A. Calcium influx
B. Potassium efflux
C. Sodium influx
D. Chloride influx
Answer: C – Fast Na⁺ entry causes rapid depolarisation. - Which of the following is false regarding phase 0?
A. It determines conduction velocity
B. It depends on fast sodium channels
C. It is calcium-mediated in ventricles
D. It produces rapid depolarisation
Answer: C – Ventricular phase 0 is sodium-mediated. - Reduction in phase 0 slope will most likely cause:
A. Faster conduction
B. Slower conduction
C. Shorter refractory period
D. Increased automaticity
Answer: B – Conduction velocity falls. - Phase 0 in SA node cells is mediated by:
A. Sodium influx
B. Potassium efflux
C. Calcium influx
D. Chloride influx
Answer: C – L-type Ca²⁺ channels dominate. - Which electrolyte disturbance most depresses phase 0?
A. Hypokalaemia
B. Hyperkalaemia
C. Hypocalcaemia
D. Hypercalcaemia
Answer: B – Sodium channel inactivation. - Which antiarrhythmic class primarily affects phase 0?
A. Class I
B. Class II
C. Class III
D. Class IV
Answer: A – Sodium channel blockers. - Which phase corresponds to the ECG QRS complex?
A. Phase 0
B. Phase 1
C. Phase 2
D. Phase 3
Answer: A – Ventricular depolarisation. - Which of the following is false about Purkinje fibres?
A. Fastest conduction
B. Large diameter
C. Calcium-dependent phase 0
D. Sodium-dependent depolarisation
Answer: C – Phase 0 is sodium-dependent. - The plateau phase is mainly due to:
A. Sodium influx
B. Calcium influx
C. Potassium influx
D. Chloride efflux
Answer: B – L-type Ca²⁺ channels. - Which phase restores resting potential?
A. Phase 1
B. Phase 2
C. Phase 3
D. Phase 4
Answer: C – Potassium efflux. - Which of the following is false regarding cardiac muscle?
A. Long refractory period
B. Plateau phase present
C. Can undergo tetany
D. Calcium-dependent contraction
Answer: C – Tetany is prevented. - Threshold for sodium channel opening is approximately:
A. −120 mV
B. −90 mV
C. −70 mV
D. −40 mV
Answer: C – Typical activation threshold. - Which current dominates phase 4 in ventricular myocytes?
A. Funny current
B. Sodium leak
C. Potassium current
D. Calcium current
Answer: C – High K⁺ permeability. - Which drug would most slow ventricular conduction?
A. Verapamil
B. Metoprolol
C. Lidocaine
D. Amiodarone
Answer: C – Sodium channel block. - Which phase overlaps with absolute refractory period?
A. Phase 4
B. Phase 3 only
C. Phases 0–2
D. Phase 1 only
Answer: C – Sodium channel inactivation. - Which ion movement ends the plateau?
A. Calcium influx
B. Sodium influx
C. Potassium efflux
D. Chloride influx
Answer: C – Repolarisation begins. - Which of the following is false?
A. Phase 0 is steep
B. Phase 2 is flat
C. Phase 3 is sodium-mediated
D. Phase 4 is stable in ventricles
Answer: C – Phase 3 is potassium-mediated. - Which structure has the slowest conduction velocity?
A. Atria
B. Purkinje fibres
C. Ventricular myocardium
D. AV node
Answer: D – AV nodal delay. - Loss of fast sodium channels would most affect:
A. SA node automaticity
B. AV nodal delay
C. Ventricular conduction
D. Plateau duration
Answer: C – Ventricular depolarisation depends on Na⁺. - Which property ensures coordinated ventricular contraction?
A. Long plateau
B. Fast Purkinje conduction
C. AV nodal delay
D. Slow atrial conduction
Answer: B – Rapid impulse distribution.
Summary for quick exam revision
The rapid depolarisation phase (phase 0) of the ventricular myocardial action potential is caused by sudden sodium influx through fast voltage-gated sodium channels. This produces the steep upstroke of the action potential and determines conduction velocity across the myocardium. Any reduction in sodium channel availability, such as with hyperkalaemia, ischaemia, or class I antiarrhythmic drugs, slows conduction and increases arrhythmic risk. Phase 0 must be clearly distinguished from nodal tissue, where calcium—not sodium—mediates depolarisation. Following phase 0, transient potassium efflux produces early repolarisation, while calcium influx during phase 2 generates the plateau that prolongs contraction and prevents tetany. Final repolarisation occurs via potassium efflux, restoring the resting membrane potential. Purkinje fibres conduct fastest due to a steep phase 0 and large fibre diameter, ensuring synchronous ventricular contraction.