A 31-year-old previously healthy man attends the medical assessment unit with a 4-day history of loose, watery stools associated with colicky abdominal pain. He returned from a large outdoor concert in England one week ago. He has no fever, no blood or mucus in stool, and is able to tolerate oral fluids. Observations are stable and abdominal examination shows only mild diffuse tenderness. Stool microscopy and culture later identify Shigella sonnei.
What is the most appropriate management at this stage?
A. Ciprofloxacin
B. Azithromycin
C. Oral rehydration therapy
D. Metronidazole
E. Amoxicillin


Correct Answer
Oral rehydration therapy
Detailed discussion for MRCP
This patient has uncomplicated shigellosis, characterised by watery (non-bloody) diarrhoea, absence of fever or systemic toxicity, stable vital signs, and preserved oral intake. In such cases, supportive management alone is sufficient, with oral rehydration forming the cornerstone of treatment.
Shigella sonnei is the most common species in the UK and other high-income countries. It typically causes milder, self-limiting illness compared with S. flexneri or S. dysenteriae, which are more often associated with severe dysentery, outbreaks, and complications. Symptoms usually resolve within 5–7 days without antibiotics.
Antibiotics are not routinely indicated in mild shigellosis because:
- Clinical benefit is minimal in uncomplicated disease
- Illness is self-limiting
- Antibiotics may prolong fecal shedding in some cases
- Rising antimicrobial resistance is a major public health concern
Antibiotic therapy is reserved for:
- Severe disease (high fever, toxicity, dehydration, frequent stools)
- Dysentery (bloody diarrhoea)
- Immunocompromised patients (HIV, transplant, chemotherapy)
- High-risk public health situations (e.g. food handlers, childcare outbreaks)
When antibiotics are required, ciprofloxacin is usually first-line in adults, with azithromycin as an alternative (especially in children, pregnancy, or fluoroquinolone resistance).
Metronidazole has no activity against Shigella as it targets anaerobes and protozoa (e.g. Entamoeba histolytica, Clostridioides difficile). Beta-lactams such as amoxicillin or co-amoxiclav are unreliable due to widespread resistance.
MRCP candidates should remember that not all positive stool cultures require antibiotics—clinical severity and host factors guide management, not microbiology alone.
Let us first go through the classification of bacteria, for exam purpose.
1. What does “bacillus” mean?
Bacillus = shape of the bacterium
Bacteria are classified by shape, just like objects:
- Cocci → round (like balls)
- Bacilli → rod-shaped (like small sticks)
- Spirilla → spiral-shaped
So when we say bacillus, it simply means:
👉 A rod-shaped bacterium
Nothing more complicated than that.
2. What does “Gram negative” mean?
This comes from a laboratory test called the Gram stain, which helps doctors identify bacteria quickly.
The Gram stain answers one question:
Does the bacterial cell wall hold a purple dye or not?
How it works (simplified):
- Bacteria are stained purple
- Then washed with alcohol
- Then counter-stained pink
Results:
- Gram positive → stays purple
- Gram negative → loses purple, turns pink
So Gram negative means:
👉 The bacterium does NOT retain the purple dye and appears pink
Why does this happen?
Because of cell wall structure:
- Gram-positive bacteria
- Thick cell wall
- No outer membrane
- Gram-negative bacteria
- Thin cell wall
- Extra outer membrane (important!)
This outer membrane:
- Contains lipopolysaccharide (LPS) → causes inflammation, fever, shock
- Makes bacteria harder to kill
- Explains antibiotic resistance
So clinically, Gram-negative = more toxic potential and treatment challenges
3. What does “non-lactose fermenter” mean?
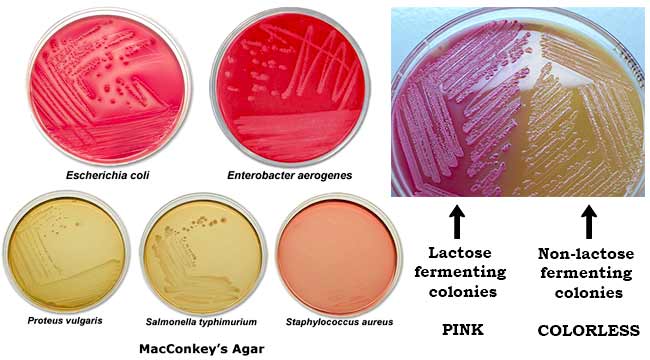
This refers to how bacteria metabolise sugar, tested using a culture medium called MacConkey agar.
Lactose = a sugar
Some bacteria can:
- Eat lactose
- Ferment it
- Produce acid
Others cannot.
On MacConkey agar:
- Lactose fermenters
- Break down lactose
- Produce acid
- Turn colonies pink
- Non-lactose fermenters
- Cannot ferment lactose
- No acid produced
- Colonies remain pale / colourless
So non-lactose fermenter means:
👉 This bacterium cannot use lactose as an energy source
Why is this important clinically?
Because it helps narrow diagnosis within hours:
- Lactose fermenters → usually gut commensals
- e.g. E. coli (often less invasive)
- Non-lactose fermenters → more likely pathogenic
- Shigella
- Salmonella
- Campylobacter
- Pseudomonas
That’s why Shigella stands out in stool cultures.
4. Putting it all together (Shigella example)
When we say:
“Shigella is a Gram-negative bacillus, non-lactose fermenter”
We mean:
- Gram-negative → has outer membrane, endotoxin, inflammatory potential
- Bacillus → rod-shaped
- Non-lactose fermenter → pathogenic gut organism, pale colonies on culture
This combination immediately tells the microbiologist and clinician:
- It’s not a harmless gut commensal
- It’s an invasive diarrhoeal pathogen
- Antibiotic choice must consider Gram-negative coverage
5. One-line memory aid
Gram negative = pink, endotoxin, outer membrane
Bacillus = rod-shaped
Non-lactose fermenter = pathogenic gut bug, pale colonies
6. Ultra-simple analogy
Think of bacteria like people:
- Shape → body type (thin, round, tall)
- Gram stain → clothing layers (single coat vs coat + jacket)
- Lactose fermentation → diet preference (can digest milk sugar or not)
Shigella:
- Stick-shaped
- Wearing an extra jacket (outer membrane)
- Cannot digest lactose
That’s all it means—no mystery.
MASTER FRAMEWORK (how your brain should approach bacteria)
Every bacterium can be classified using 5 simple questions:
- Gram stain → Positive or Negative?
- Shape → Cocci or Bacilli?
- Oxygen requirement → Aerobic or Anaerobic?
- Special features → Spores? Acid-fast? Intracellular?
- Clinical setting → Skin, gut, lung, hospital, zoonotic?
We’ll now build this step by step, from simple to complex.
1️⃣ CLASSIFICATION BY SHAPE (FIRST LOOK UNDER MICROSCOPE)
A. Cocci (round)
- Staphylococcus
- Streptococcus
- Enterococcus
- Neisseria
B. Bacilli (rods)
- E. coli
- Shigella
- Salmonella
- Klebsiella
- Pseudomonas
- Clostridium
- Mycobacterium
C. Curved / Spiral
- Vibrio
- Campylobacter
- Helicobacter
- Spirochetes (Treponema, Leptospira)



2️⃣ GRAM STAIN CLASSIFICATION (MOST IMPORTANT CLINICALLY)
🟣 GRAM POSITIVE (purple)
Thick cell wall, no outer membrane
A. Gram-positive cocci
- Staphylococcus (clusters)
- Streptococcus (chains)
- Enterococcus
B. Gram-positive bacilli
- Spore-forming
- Bacillus (aerobic)
- Clostridium (anaerobic)
- Non-spore-forming
- Listeria
- Corynebacterium
🔴 GRAM NEGATIVE (pink)
Thin wall + outer membrane (endotoxin!)
A. Gram-negative cocci
- Neisseria (gonorrhoeae, meningitidis)
B. Gram-negative bacilli
- Enterobacteriaceae (gut bugs)
- Non-fermenters (hospital bugs)
- Curved rods



3️⃣ GRAM-POSITIVE BACTERIA — CLEAN & SIMPLE
Gram-positive cocci
| Pattern | Organism | Typical disease |
|---|---|---|
| Clusters | Staphylococcus aureus | Skin, abscess, endocarditis |
| Chains | Streptococcus | Tonsillitis, rheumatic fever |
| Pairs | Enterococcus | UTI, endocarditis |
Gram-positive bacilli
| Feature | Organism | Key disease |
|---|---|---|
| Spore + aerobic | Bacillus anthracis | Anthrax |
| Spore + anaerobic | Clostridium | Tetanus, gas gangrene |
| No spores | Listeria | Neonatal sepsis |
| Club-shaped | Corynebacterium | Diphtheria |
4️⃣ GRAM-NEGATIVE BACTERIA — HIGH-YIELD ORGANISATION
A. Enterobacteriaceae (gut bacilli)
All are:
- Gram negative bacilli
- Facultative anaerobes
- From gut
Lactose fermenters (pink on MacConkey)
- E. coli
- Klebsiella
- Enterobacter
Non-lactose fermenters (pale)
- Shigella
- Salmonella
- Proteus
- Yersinia

B. Non-fermenters (hospital nightmares)
| Organism | Clue |
|---|---|
| Pseudomonas | ICU, ventilators, burns |
| Acinetobacter | MDR, hospital outbreaks |
| Stenotrophomonas | Immunocompromised |
C. Curved Gram-negative rods
| Organism | Disease |
|---|---|
| Vibrio cholerae | Profuse watery diarrhoea |
| Campylobacter | Bloody diarrhoea |
| Helicobacter pylori | Peptic ulcer |
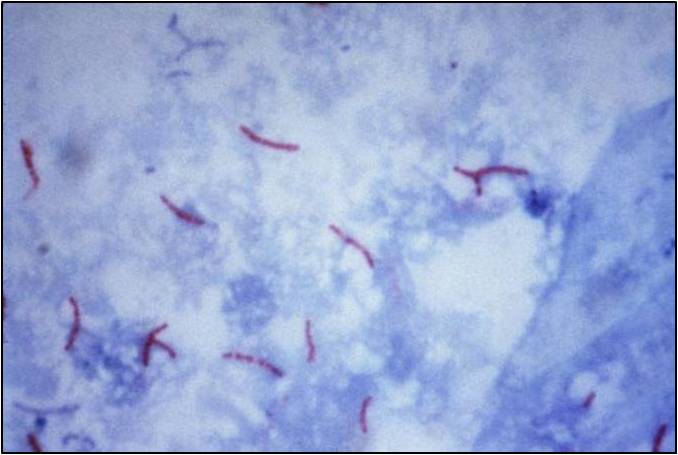
5️⃣ ACID-FAST BACTERIA (SPECIAL STAINS)
| Organism | Why special? |
|---|---|
| Mycobacterium tuberculosis | Waxy cell wall |
| Mycobacterium leprae | Nerve involvement |
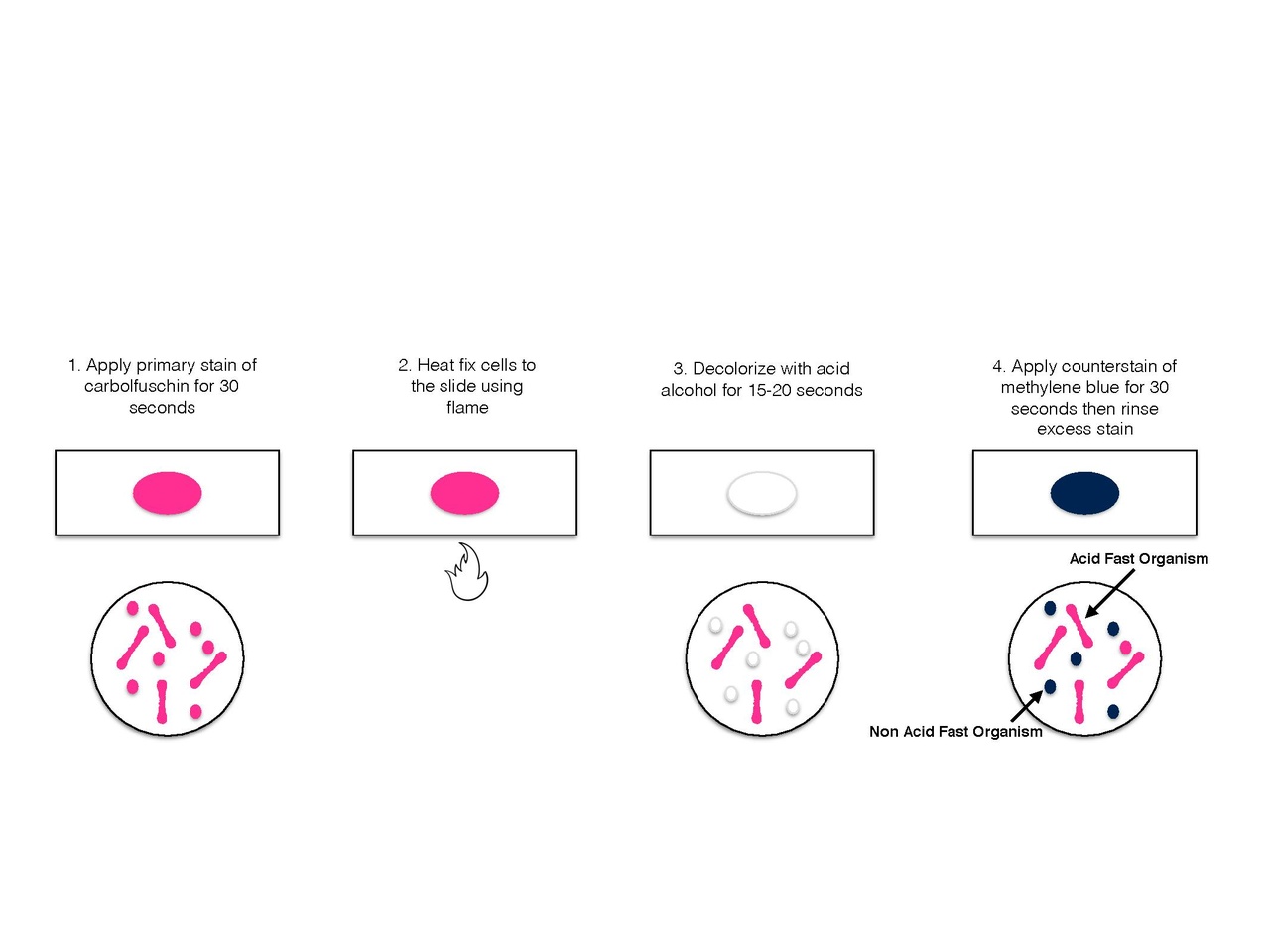
- Do NOT Gram stain well
- Need Ziehl–Neelsen stain

6️⃣ ANAEROBES (THINK: NO OXYGEN)
Gram-positive anaerobes
- Clostridium (most important)
Gram-negative anaerobes
- Bacteroides
- Fusobacterium
Clinical clue: foul smell, abscess, necrotic tissue
7️⃣ INTRACELLULAR & ATYPICAL BACTERIA
| Organism | Key feature |
|---|---|
| Chlamydia | No peptidoglycan |
| Mycoplasma | No cell wall |
| Rickettsia | Obligate intracellular |
| Legionella | Water systems |
They do not respond to beta-lactams
8️⃣ ONE-PAGE EXAM TABLE (GOLD)
| Category | Think |
|---|---|
| Gram + cocci | Skin & throat |
| Gram + bacilli | Toxins |
| Gram – bacilli | Gut & hospital |
| Non-lactose fermenter | Pathogenic |
| Anaerobe | Abscess |
| Acid-fast | TB |
| No cell wall | Mycoplasma |
9️⃣ SUPER-HIGH-YIELD MEMORY LINE
Gram positive = purple walls
Gram negative = pink + endotoxin
Cocci = round
Bacilli = rods
Non-lactose fermenter = pathogen
Anaerobe = abscess
Acid-fast = TB
10️⃣ FINAL BIG PICTURE (how consultants think)
When a report says:
“Gram-negative bacillus, non-lactose fermenter”
Your brain should instantly say:
- Pathogenic gut or hospital organism
- Likely invasive
- Antibiotics must cover Gram-negative bugs
- Avoid beta-lactams blindly
Now let us talk about endo and exotoxins.
1️⃣ Endotoxin — ONLY Gram-negative
What is endotoxin?
- Lipopolysaccharide (LPS)
- Located in the outer membrane of Gram-negative bacteria
- The toxic part is Lipid A
Who has endotoxin?
✅ Only Gram-negative bacteria
Why?
- Only Gram-negative bacteria have an outer membrane
- Gram-positive bacteria do not have LPS at all
Clinical effects of endotoxin
- Fever
- Hypotension
- Septic shock
- DIC
These occur because LPS strongly activates:
- Macrophages
- TNF-α, IL-1, IL-6
- Complement and coagulation cascades
So:
Gram-negative = endotoxin (always)
2️⃣ Exotoxin — BOTH Gram-positive AND Gram-negative
What is an exotoxin?
- A protein toxin
- Actively secreted by bacteria
- Often very potent and specific
Who can produce exotoxins?
✅ Both Gram-positive AND Gram-negative bacteria
Exotoxin production has nothing to do with Gram stain.
3️⃣ High-yield examples
Gram-positive exotoxins
| Organism | Exotoxin |
|---|---|
| Staphylococcus aureus | Enterotoxin, TSST-1 |
| Streptococcus pyogenes | Streptolysin, erythrogenic toxin |
| Clostridium tetani | Tetanospasmin |
| Clostridium botulinum | Botulinum toxin |
| Corynebacterium diphtheriae | Diphtheria toxin |
Gram-negative exotoxins
| Organism | Exotoxin |
|---|---|
| Vibrio cholerae | Cholera toxin |
| Shigella dysenteriae | Shiga toxin |
| E. coli | LT, ST, Shiga-like toxin |
| Pseudomonas aeruginosa | Exotoxin A |
| Bordetella pertussis | Pertussis toxin |
So:
Exotoxins are NOT exclusive to Gram-positive bacteria
4️⃣ Key differences: Endotoxin vs Exotoxin (EXAM GOLD)
| Feature | Endotoxin | Exotoxin |
|---|---|---|
| Chemical nature | Lipopolysaccharide | Protein |
| Location | Cell wall (outer membrane) | Secreted |
| Found in | Gram-negative only | Gram+ and Gram− |
| Heat stability | Heat stable | Heat labile |
| Specificity | Non-specific | Highly specific |
| Antigenicity | Weak | Strong |
| Can be made into vaccine | ❌ No | ✅ Yes (toxoid) |
| Causes fever & shock | Very common | Sometimes |
5️⃣ One-line MRCP rule (write this in your brain)
All Gram-negative bacteria have endotoxin (LPS), but exotoxins can be produced by both Gram-positive and Gram-negative bacteria.
6️⃣ Ultra-simple mental model
Think of bacteria like people:
- Endotoxin = toxic jacket they are wearing
- Only Gram-negative people wear this jacket
- It harms you when the person breaks apart
- Exotoxin = weapon they actively throw
- Anyone (Gram+ or Gram−) can throw it
- Often very precise and dangerous
7️⃣ Why this matters clinically (consultant-level thinking)
- Septic shock with DIC → think Gram-negative endotoxin
- Toxin-mediated syndromes (tetanus, botulism, cholera) → exotoxin
- Vaccines against diphtheria & tetanus → toxoid vaccines
- Killing Gram-negative bacteria can initially worsen shock → endotoxin release
Final take-home sentence
Gram-negative bacteria are defined by endotoxin (LPS), not by exotoxin production — exotoxins are shared by both Gram-positive and Gram-negative organisms.
Now let us find out what cytokines are.
When bacteria (especially Gram-negative LPS) enter the body, the immune system releases chemical messengers to warn, recruit, and activate defenses.
These messengers are called cytokines.
Among them, the most important are:
- TNF-α
- Interleukins (IL-1, IL-6, etc.)
They are signals, not cells.
Think of them as WhatsApp messages between immune cells.
1️⃣ What is TNF-α (Tumour Necrosis Factor-alpha)?
In very simple words:
TNF-α is the body’s emergency alarm signal.
Who produces TNF-α?
- Mainly macrophages
- Also T cells, NK cells
When is it released?
- When macrophages see danger:
- LPS (endotoxin)
- Bacteria
- Severe infection
- Tissue damage
What does TNF-α do?
Think of TNF as shouting:
“THERE IS A SERIOUS INFECTION — ALL HANDS ON DECK!”
It causes:
- Fever
- Vasodilation → low BP
- Capillary leak → oedema
- Activation of coagulation → DIC
- Recruitment of more immune cells
Too much TNF-α = disaster
| Level | Effect |
|---|---|
| Small | Helps fight infection |
| Excessive | Septic shock |
| Uncontrolled | DIC, organ failure, death |
That’s why Gram-negative sepsis is so dangerous.
2️⃣ What are Interleukins (ILs)?
Simple definition:
Interleukins are communication molecules between white blood cells.
“Inter-leukin” literally means:
Between leukocytes (white cells)
They help immune cells talk to each other.
3️⃣ Important interleukins you MUST know (MRCP core)
🔹 IL-1
Role: Fever and inflammation
- Raises body temperature
- Activates endothelium
- Helps T-cell activation
👉 IL-1 = “Turn up the heat”
🔹 IL-6
Role: Acute phase response
- Stimulates liver to make:
- CRP
- Fibrinogen
- Ferritin
- Causes fever
- Links infection to lab markers
👉 IL-6 = “Make CRP rise”
This is why:
- CRP ↑ in sepsis
- IL-6 blockers reduce inflammation
🔹 IL-8 (bonus, very useful)
Role: Neutrophil recruitment
- Brings neutrophils to site of infection
👉 IL-8 = “Call the neutrophils”
4️⃣ Putting TNF + ILs together (very high yield)
When LPS enters blood:
- Macrophages get activated
- They release:
- TNF-α
- IL-1
- IL-6
- These cause:
- Fever
- Hypotension
- Capillary leak
- Raised CRP
- DIC
That entire picture = sepsis
5️⃣ Complement cascade (simple explanation)
What is complement?
A group of proteins in blood that:
- Punch holes in bacteria
- Enhance inflammation
- Attract immune cells
What activates complement?
- LPS
- Antigen–antibody complexes
Effects:
- Cell lysis
- Inflammation
- Vascular permeability
Complement + TNF together worsen shock.
6️⃣ Coagulation cascade activation (why DIC happens)
TNF and IL-1:
- Activate tissue factor
- Suppress anticoagulant pathways
- Cause widespread microthrombi
Result:
- Clotting + bleeding at same time
- ↓ Platelets
- ↑ D-dimer
- ↓ Fibrinogen
That is DIC.
7️⃣ One diagram in words (store this mentally)
LPS → macrophage → TNF + IL-1 + IL-6 →
- Fever
- Low BP
- Capillary leak
- ↑ CRP
- Coagulation activation
- DIC
8️⃣ Ultra-high-yield exam summary (memorise this)
- TNF-α → shock, hypotension, DIC
- IL-1 → fever
- IL-6 → CRP & acute phase response
- IL-8 → neutrophils
- LPS → macrophage activation
- Gram-negative sepsis → cytokine storm
9️⃣ Consultant-level one-liner
Endotoxin doesn’t kill directly — it kills by forcing the immune system to overreact via TNF and interleukins.
10️⃣ If you remember only ONE sentence
TNF and interleukins are chemical messengers released by immune cells that cause fever, inflammation, shock, and DIC during severe infection.
Cheat sheet (exam-focused)
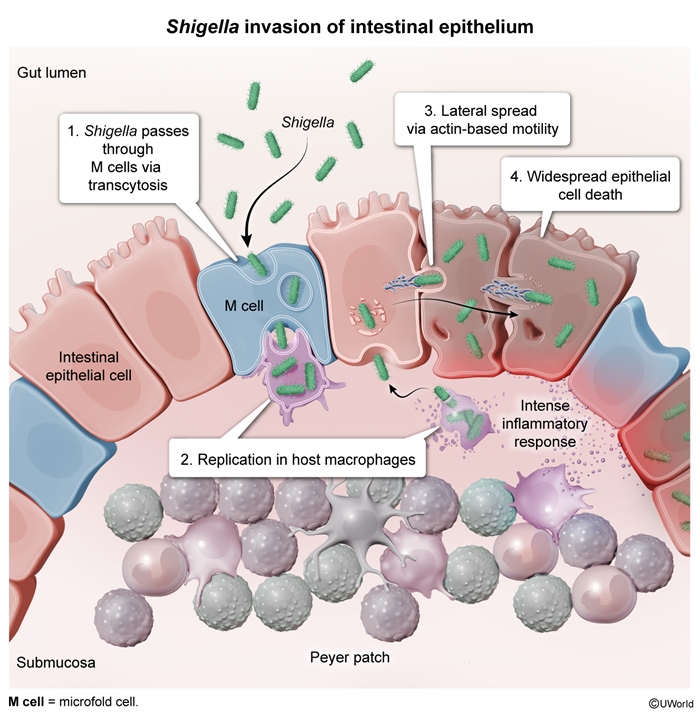
- Organism: Shigella (Gram-negative, non-motile bacillus)
- Transmission: Fecal–oral, low infectious dose
- UK most common species: S. sonnei
- Typical symptoms: Diarrhoea, abdominal cramps ± fever
- Bloody diarrhoea suggests severe disease
- Mild disease → supportive care only
- Mainstay of treatment: Oral rehydration
- Antibiotics only if severe, bloody, immunocompromised
- First-line antibiotic (if needed): Ciprofloxacin
- Alternative: Azithromycin
- Metronidazole: no role
- Beta-lactams: high resistance
- Complications: dehydration, seizures (children), reactive arthritis
- Public health: notify if outbreaks or high-risk occupations
Flash cards
Q1: What type of diarrhoea does uncomplicated shigellosis usually cause?
A: Watery diarrhoea.
Explanation: Bloody diarrhoea indicates more severe disease.
Q2: Most common Shigella species in the UK?
A: Shigella sonnei.
Explanation: Causes milder illness than other species.
Q3: Primary treatment for mild shigellosis?
A: Oral rehydration therapy.
Explanation: Disease is self-limiting.
Q4: When are antibiotics indicated in Shigella infection?
A: Severe disease, dysentery, immunocompromised patients.
Explanation: Routine use is discouraged.
Q5: First-line antibiotic for severe Shigella in adults?
A: Ciprofloxacin.
Explanation: Effective against Gram-negative enteric bacteria.
Q6: Why avoid antibiotics in mild disease?
A: Resistance and minimal clinical benefit.
Explanation: May prolong bacterial shedding.
Q7: Does metronidazole treat Shigella?
A: No.
Explanation: Targets anaerobes and protozoa.
Q8: Gram stain of Shigella?
A: Gram-negative bacillus.
Explanation: Non-lactose fermenter.
Q9: Infectious dose of Shigella—high or low?
A: Very low.
Explanation: Explains outbreak potential.
Q10: Typical duration of illness without antibiotics?
A: 5–7 days.
Explanation: Self-limiting.
Q11: Which species causes most severe disease worldwide?
A: Shigella dysenteriae.
Explanation: Associated with dysentery and toxins.
Q12: Key public health concern with Shigella?
A: Antimicrobial resistance.
Explanation: Especially fluoroquinolone resistance.
Q13: Can Shigella cause reactive arthritis?
A: Yes.
Explanation: Post-infectious complication.
Q14: Main risk of dehydration in Shigella?
A: Young children and elderly.
Explanation: Reduced physiological reserve.
Q15: Stool finding that mandates antibiotics?
A: Blood.
Explanation: Indicates invasive disease.
Q16: Should asymptomatic carriers be treated?
A: Usually no.
Explanation: Except in public health-sensitive roles.
Q17: Mechanism of disease—enterotoxin or invasion?
A: Mucosal invasion.
Explanation: Causes inflammation and ulceration.
Q18: Preferred therapy in pregnancy if antibiotics needed?
A: Azithromycin.
Explanation: Avoid fluoroquinolones.
Q19: Is fever mandatory for Shigella diagnosis?
A: No.
Explanation: Mild cases may be afebrile.
Q20: Key MRCP principle in infective diarrhoea?
A: Treat the patient, not the culture.
Explanation: Severity determines therapy.
MCQs to test yourself
1. In uncomplicated Shigella infection, the most appropriate management is:
A. Ciprofloxacin
B. Oral rehydration therapy
C. Metronidazole
D. Co-amoxiclav
E. Loperamide alone
Answer: B – Supportive care is sufficient
2. Which feature most strongly indicates the need for antibiotics in shigellosis?
A. Watery stools
B. Recent travel to the UK
C. Bloody diarrhoea
D. Mild abdominal pain
E. Normal observations
Answer: C – Suggests invasive disease
3. Shigella sonnei infection is typically:
A. Fulminant and toxic
B. Self-limiting and mild
C. Always bloody
D. Anaerobic
E. Protozoal
Answer: B – Mild illness
4. Which antibiotic has no role in Shigella infection?
A. Ciprofloxacin
B. Azithromycin
C. Ceftriaxone
D. Metronidazole
E. Trimethoprim
Answer: D – Ineffective
5. Which statement is false regarding Shigella?
A. Low infectious dose
B. Gram-negative bacillus
C. Causes self-limiting disease
D. Always requires antibiotics
E. Can cause outbreaks
Answer: D – Antibiotics not always required
6. First-line antibiotic in severe adult shigellosis:
A. Amoxicillin
B. Metronidazole
C. Ciprofloxacin
D. Doxycycline
E. Vancomycin
Answer: C
7. The mainstay of treatment in mild disease is:
A. IV antibiotics
B. IV fluids only
C. Oral rehydration
D. Steroids
E. Antidiarrhoeals
Answer: C
8. Which group should always be considered for antibiotics?
A. Healthy adults
B. Children with mild diarrhoea
C. Immunocompromised patients
D. Afebrile patients
E. UK residents
Answer: C
9. Shigella primarily causes disease by:
A. Toxin-mediated secretion
B. Viral cytopathy
C. Mucosal invasion
D. Anaerobic fermentation
E. Biofilm formation
Answer: C
10. Which is false regarding antibiotic use in Shigella?
A. Reduces duration in severe disease
B. Needed in all cases
C. Promotes resistance if overused
D. Reserved for dysentery
E. Depends on host factors
Answer: B
Now let us do some more MCQs to test our knowledge of immune response-
1.
The primary determinant of the Gram stain reaction is the:
A. Presence of lipopolysaccharide
B. Thickness of peptidoglycan layer
C. Ability to form spores
D. Presence of flagella
E. Ability to ferment glucose
Correct answer: B
Detailed explanation:
Gram staining depends on the ability of the bacterial cell wall to retain crystal violet–iodine complex during alcohol decolourisation.
- Gram-positive bacteria have a thick peptidoglycan layer, which traps the dye.
- Gram-negative bacteria have a thin peptidoglycan layer and lose the dye, taking up safranin instead.
This structural difference—not metabolism or motility—is the key determinant.
2.
Which structural component is unique to gram-negative bacilli and absent in gram-positive bacteria?
A. Teichoic acid
B. Peptidoglycan
C. Outer membrane
D. Cytoplasmic membrane
E. Ribosomes
Correct answer: C
Detailed explanation:
The outer membrane is a defining feature of gram-negative bacteria.
- It contains lipopolysaccharide (LPS), porins, and phospholipids.
- Gram-positive organisms lack an outer membrane but contain teichoic acids instead.
This outer membrane explains intrinsic antibiotic resistance and endotoxin-related inflammation.
3.
Lipopolysaccharide (LPS) is best described as:
A. An exotoxin actively secreted by bacteria
B. A protein toxin causing enzymatic damage
C. A structural component released on bacterial lysis
D. A capsule polysaccharide
E. A flagellar protein
Correct answer: C
Detailed explanation:
LPS is an endotoxin, not an exotoxin.
- It is a structural component of the outer membrane
- It is released when bacteria die, lyse, or divide
Unlike exotoxins, it is not actively secreted and does not have enzymatic activity.
4.
Which portion of LPS is primarily responsible for cytokine release?
A. O antigen
B. Core polysaccharide
C. Lipid A
D. Peptidoglycan
E. Porin protein
Correct answer: C
Detailed explanation:
Lipid A is the toxic, biologically active component of LPS.
- It binds immune receptors and triggers TNF-α, IL-1, and IL-6 release
- O antigen is important for serotyping, not toxicity
This is a high-yield MRCP concept.
5.
Which immune cell is the principal initiator of cytokine release in response to endotoxin?
A. Neutrophil
B. Eosinophil
C. Macrophage
D. B lymphocyte
E. Plasma cell
Correct answer: C
Detailed explanation:
Macrophages are the central innate immune cells responding to endotoxin.
They express TLR4 receptors, recognise Lipid A, and release pro-inflammatory cytokines.
Neutrophils respond later; lymphocytes are part of adaptive immunity.
6.
Endotoxin (lipopolysaccharide) from gram-negative bacilli initiates the innate immune response by binding to a specific receptor complex.
On which receptor complex, and on which cell type, does this interaction primarily occur?
A. TLR2 on neutrophils
B. TLR4–CD14 complex on macrophages
C. Fcγ receptor on B lymphocytes
D. Complement C3b receptor on erythrocytes
E. MHC class I molecules on all nucleated cells
Correct answer: B
Lipopolysaccharide (LPS), specifically its Lipid A component, is recognised by the innate immune system, not the adaptive immune system.
🔹 Receptor Complex
The TLR4–CD14–MD2 receptor complex is responsible for detecting LPS.
-
TLR4 (Toll-like receptor 4) is the key pattern-recognition receptor
-
CD14 acts as a co-receptor that facilitates LPS binding
-
MD2 stabilises the interaction with Lipid A
🔹 Cell Type
This receptor complex is primarily expressed on:
-
Macrophages (most important)
-
Monocytes
-
Dendritic cells
Macrophages are the central initiators of cytokine release in endotoxin exposure.
🔹 Downstream Effects
Once LPS binds to the TLR4–CD14 complex on macrophages:
-
NF-κB signalling pathway is activated
-
Rapid release of TNF-α, IL-1, and IL-6 occurs
-
This leads to fever, vasodilation, capillary leak, hypotension, and shock in severe cases
7.
Which cytokine is the earliest and most central mediator of endotoxin-induced shock?
A. IL-4
B. IL-10
C. TNF-α
D. IL-17
E. IFN-γ
Correct answer: C
Detailed explanation:
TNF-α is released early and drives:
- Fever
- Vasodilation
- Capillary leak
- Hypotension
Blocking TNF-α experimentally prevents septic shock—highlighting its central role.
8.
Which cytokine is most responsible for fever via hypothalamic action?
A. IL-1
B. IL-2
C. IL-5
D. IL-8
E. TGF-β
Correct answer: A
Detailed explanation:
IL-1 acts on the hypothalamus to increase prostaglandin E₂, raising the temperature set-point.
TNF-α also contributes, but IL-1 is classically linked to pyrexia.
9.
Excessive cytokine release in severe infection is best termed:
A. Hypersensitivity reaction
B. Immune tolerance
C. Cytokine storm
D. Molecular mimicry
E. Immune paralysis
Correct answer: C
Detailed explanation:
A cytokine storm refers to uncontrolled release of inflammatory mediators causing systemic inflammation, shock, and organ failure.
10.
Which cytokine is primarily responsible for neutrophil chemotaxis?
A. IL-2
B. IL-6
C. IL-8
D. IL-12
E. IL-18
Correct answer: C
Detailed explanation:
IL-8 is a potent chemokine attracting neutrophils to infection sites—key for acute inflammation.
11.
Which feature best differentiates endotoxin from exotoxin?
A. Heat stability
B. Protein structure
C. Enzymatic activity
D. High antigenicity
E. Ability to form toxoids
Correct answer: A
Detailed explanation:
Endotoxins are heat stable, non-protein molecules.
Exotoxins are heat-labile proteins and can be converted into toxoids (e.g. vaccines).
12.
Which statement about exotoxins is FALSE?
A. They are actively secreted
B. They are usually proteins
C. They can be converted to toxoids
D. They commonly cause septic shock
E. They are highly antigenic
Correct answer: D
Detailed explanation:
Septic shock is classically endotoxin-mediated.
Exotoxins cause specific tissue damage, not systemic shock.
13.
Which bacterial classification is based on oxygen requirement?
A. Gram stain
B. Shape
C. Acid-fastness
D. Aerobic vs anaerobic
E. Capsule formation
Correct answer: D
Detailed explanation:
Oxygen requirement divides bacteria into obligate aerobes, obligate anaerobes, facultative anaerobes, etc.—clinically important for infection site prediction.
14.
Which category includes organisms that survive without oxygen but use it if available?
A. Obligate aerobes
B. Obligate anaerobes
C. Facultative anaerobes
D. Microaerophiles
E. Capnophiles
Correct answer: C
Detailed explanation:
Facultative anaerobes are metabolically flexible—important clinically because they thrive in diverse tissues.
15.
Which bacterial shape classification correctly matches gram-negative bacilli?
A. Cocci in chains
B. Cocci in clusters
C. Rod-shaped organisms
D. Spiral-shaped organisms
E. Filamentous organisms
Correct answer: C
Detailed explanation:
“Bacillus” means rod-shaped—shape is independent of Gram reaction but often tested together.
16.
Which laboratory feature best indicates lactose fermentation?
A. Growth on blood agar
B. Colour change on MacConkey agar
C. Catalase positivity
D. Coagulase positivity
E. Oxidase positivity
Correct answer: B
Detailed explanation:
MacConkey agar differentiates lactose fermenters (pink colonies) from non-fermenters (pale colonies).
17.
Which host response directly causes hypotension in endotoxin-mediated shock?
A. Antibody production
B. Complement fixation
C. Nitric oxide–mediated vasodilation
D. Platelet aggregation
E. T-cell apoptosis
Correct answer: C
Detailed explanation:
Cytokines induce nitric oxide release, causing profound vasodilation and shock.
18.
Which cytokine primarily stimulates hepatic acute-phase protein synthesis?
A. IL-2
B. IL-4
C. IL-6
D. IL-8
E. IL-13
Correct answer: C
Detailed explanation:
IL-6 stimulates production of CRP, fibrinogen, and serum amyloid A.
19.
Which bacterial component contributes most to intrinsic antibiotic resistance in gram-negative bacilli?
A. Peptidoglycan
B. Capsule
C. Outer membrane
D. Ribosome
E. Flagellum
Correct answer: C
Detailed explanation:
The outer membrane limits drug penetration—explaining resistance to many β-lactams.
20.
Which laboratory finding is most directly cytokine-mediated?
A. Raised bilirubin
B. Elevated C-reactive protein
C. Reduced calcium
D. Metabolic alkalosis
E. Thrombocytosis
Correct answer: B
Detailed explanation:
CRP is directly induced by IL-6 and is a marker of systemic inflammation.
“Now let us do some MCQs in the format- which of the following is FALSE?”
21.
Regarding gram-negative bacterial cell walls, which statement is FALSE?
A. They contain an outer membrane
B. They contain lipopolysaccharide
C. They have thick peptidoglycan layers
D. They possess porin channels
E. They stain pink on Gram stain
Answer: C
22.
Regarding endotoxin, which statement is FALSE?
A. It is heat stable
B. It is a protein toxin
C. It triggers cytokine release
D. It is part of the bacterial cell wall
E. It is released on bacterial lysis
Answer: B
23.
Regarding TNF-α, which statement is FALSE?
A. It causes fever
B. It increases vascular permeability
C. It causes hypotension
D. It suppresses inflammation
E. It contributes to septic shock
Answer: D
24.
Regarding IL-6, which statement is FALSE?
A. It induces acute-phase proteins
B. It causes CRP elevation
C. It is anti-inflammatory only
D. It contributes to fever
E. It is produced by macrophages
Answer: C
25.
Regarding exotoxins, which statement is FALSE?
A. They are proteins
B. They are actively secreted
C. They can be converted into toxoids
D. They are weakly antigenic
E. They have specific targets
Answer: D
26.
Regarding bacterial classification, which statement is FALSE?
A. Shape classification includes cocci and bacilli
B. Oxygen requirement is clinically relevant
C. Gram stain reflects cell wall structure
D. Capsule presence affects virulence
E. All gram-negative bacteria are anaerobic
Answer: E
27.
Regarding cytokines, which statement is FALSE?
A. They mediate cell-to-cell signalling
B. They are produced only by lymphocytes
C. They can cause systemic effects
D. They are central to inflammation
E. They can cause fever
Answer: B
28.
Regarding endotoxin-induced shock, which statement is FALSE?
A. It involves nitric oxide release
B. It causes vasodilation
C. It causes capillary leak
D. It is mediated primarily by antibodies
E. It may cause multi-organ failure
Answer: D
29.
Regarding MacConkey agar, which statement is FALSE?
A. It is selective for gram-negative bacteria
B. It differentiates lactose fermentation
C. It contains bile salts
D. It supports gram-positive growth well
E. It is commonly used in stool cultures
Answer: D
30.
Regarding gram-negative bacilli, which statement is FALSE?
A. They possess an outer membrane
B. They contain lipopolysaccharide
C. They are always spore-forming
D. They trigger innate immune responses
E. They often activate cytokine cascades
Answer: C
Summary for quick exam revision
Shigella infection commonly causes self-limiting gastroenteritis, particularly Shigella sonnei in the UK, which typically presents with watery diarrhoea and mild abdominal pain. In haemodynamically stable, immunocompetent patients without fever or bloody stools, antibiotics are not indicated. Oral rehydration therapy is the cornerstone of management and is sufficient in uncomplicated disease. Antibiotics are reserved for severe illness, dysentery, immunocompromised patients, or specific public health situations. Ciprofloxacin is first-line when treatment is required, with azithromycin as an alternative. Metronidazole has no role in Shigella infection. Overuse of antibiotics contributes to resistance and may prolong bacterial shedding. MRCP candidates should focus on severity-based management rather than treating microbiology results alone.